

The earlobe device for anxiety, depression & insomnia — what does the science actually say?
A clear and clinician-level guide to cranial electrotherapy stimulation and how it stacks up against medication

Somewhere between a wellness podcast and a Reddit thread, many people have discovered a device that clips to their earlobes, sends a gentle electrical current through their brain, and promises to calm anxiety, lift depression, and fix their sleep without medication.
The technology underneath it is called cranial electrotherapy stimulation, or CES - the most well-known brand being Alpha-Stim. This article aims to cut through both the hype and the dismissiveness. We will look at what CES actually is, what the clinical trials show, how it compares to standard medications, and what a thoughtful, evidence-informed take on it looks like — whether you are a clinician deciding whether to discuss it with clients, or a curious person trying to figure out if a $700 device is worth it.
What is CES, and what does it actually do?
CES is not a new idea. Devices using low-level alternating electrical current applied to the head have been studied since the 1960s. Alpha-Stim, the dominant brand in the current market, uses a proprietary 0.5 Hz waveform delivered through ear clip electrodes at currents typically between 100–500 microamps; far below the threshold that produces any sensation of shock. Most sessions run 20–60 minutes.
CES is not electroconvulsive therapy (ECT) and not transcranial magnetic stimulation (TMS). Both of those involve much higher energy and are administered in clinical settings. CES is a consumer-accessible device, available by prescription in some states and over-the-counter in others, that people use at home. The retail price is roughly $500–$900.
The FDA cleared Alpha-Stim and similar devices under a grandfather provision that predates modern randomized trial requirements. This means FDA clearance, by itself, does not tell us whether the device works — it tells us it was deemed similar enough to an earlier device to be sold. The clinical evidence is a separate question, and it is where things get interesting.
What the research shows: a condition-by-condition breakdown
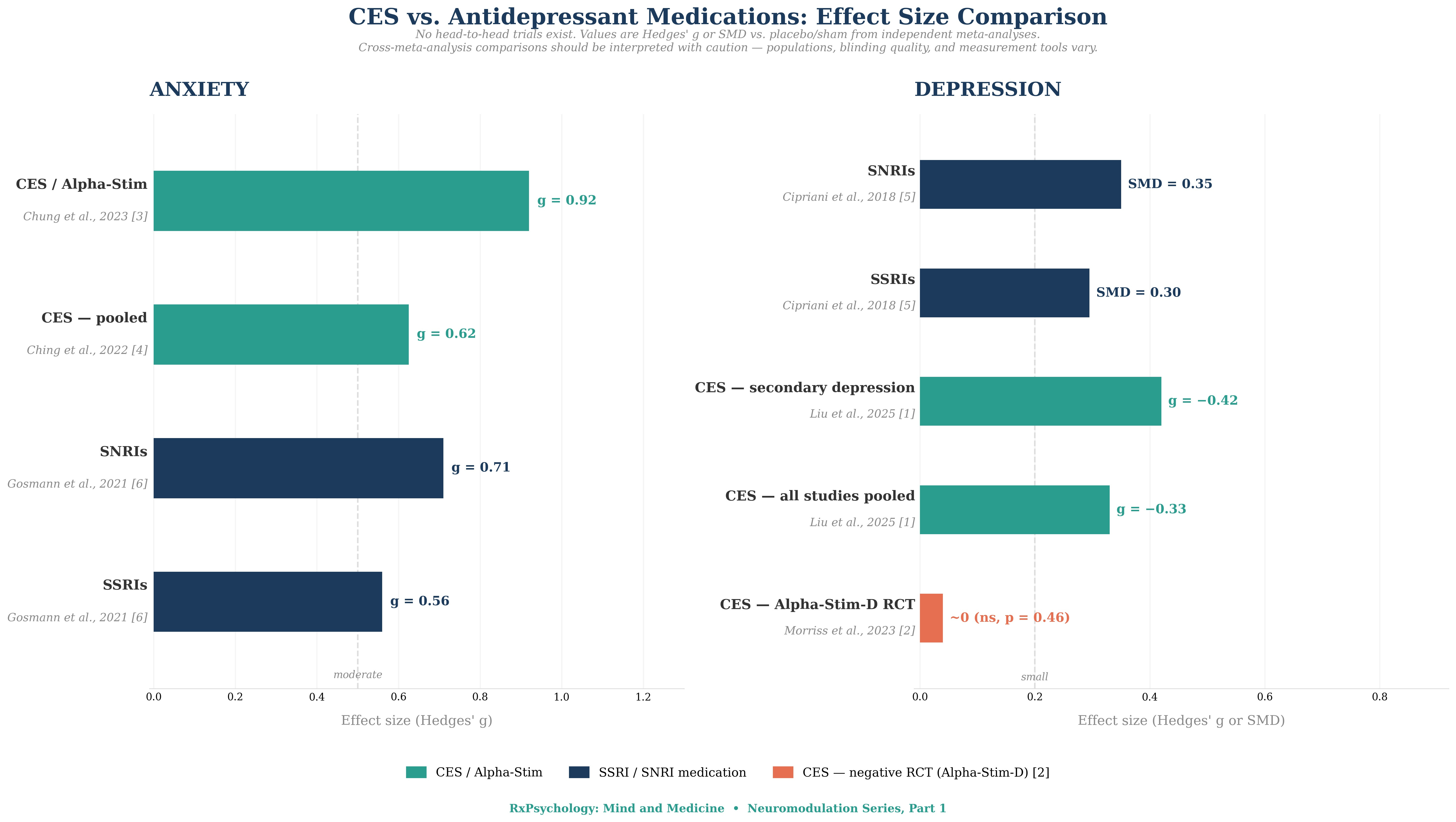
Figure 1. Effect size comparison: CES vs. antidepressant medications for anxiety and depression. Sources: Chung et al. (2023) [3]; Ching et al. (2022) [4]; Cipriani et al. (2018) [5]; Gosmann et al. (2021) [6]; Liu et al. (2025) [1]; Morriss et al. (2023) [2]; Cheng et al. (2022) [9]. All values are Hedges’ g or SMD vs. placebo/sham. No direct head-to-head CES vs. medication trials exist.
Anxiety — the strongest signal
Here is where the story gets surprising: in effect size comparisons, CES for anxiety performs as well as or better than first-line antidepressants. A 2023 meta-analysis of 8 RCTs (N = 337) found CES reduced anxiety with a large effect size of −0.96, with Alpha-Stim specifically showing an effect size of −0.88 across 4 trials.[3] A 2022 meta-analysis of 11 RCTs (N = 692) reported a moderate effect of g = −0.63.[4] A separate 2022 comparative neuromodulation meta-analysis found CES had an effect size of g = 0.711 for anxiety.[9]
By comparison, SSRIs and SNRIs — the standard first-line medications for anxiety disorders — show effect sizes of approximately 0.56–0.71 in large meta-analyses.[6] On this metric alone, CES for anxiety is not obviously inferior to medication.
Important nuance
Effect size comparisons across different meta-analyses are not the same as head-to-head trials. The populations, measurement tools, blinding quality, and baseline severity all differ. No study has yet directly randomized patients to CES versus an SSRI. We can observe that the numbers sit in a comparable range — we cannot conclude equivalence. That said, it is a compelling picture.
Depression — where the evidence gets complicated
This is the most important section for anyone considering CES primarily for depression — and it is where the gap between marketing and evidence is widest.
When you pool all available studies, CES shows a small effect size for depression (g = −0.33 overall; g = −0.42 for secondary depression comorbid with other conditions).[1] A separate meta-analysis reported a higher pooled effect of g = 0.654, though this combined clinical and non-clinical populations.[9] On the surface, those numbers look roughly comparable to SSRIs (SMD 0.27–0.32) and SNRIs (SMD 0.33–0.37) from the landmark Cipriani et al. (2018) network meta-analysis of 116,477 participants.[5] But there is a critical problem: the best individual study contradicts it entirely.
The Alpha-Stim-D trial, published in The Lancet Psychiatry in 2023, was the largest, most rigorously designed CES trial ever conducted — 236 adults with major depressive disorder, double-blind, with verified sham control, in UK primary care. The result: no significant difference between active Alpha-Stim and sham (HDRS-17 difference = −0.6, p = 0.46).[2] The device did not outperform a placebo in a well-controlled, independently funded study.
Why this matters
When pooled meta-analyses show a positive effect, but the largest rigorous trial is flat, it usually signals that smaller studies were biased by inadequate blinding, publication bias, or conflicts of interest. The Alpha-Stim-D trial was independently funded and pre-registered. Its negative result carries significant corrective weight against the pooled literature.[2]
Where might CES still help with depression? The evidence is modestly better for secondary depression — depressive symptoms comorbid with anxiety or a chronic medical condition — where effect sizes rise to around g = −0.42.[1] This makes biological sense: if anxiety is the primary driver, addressing anxiety may lift mood as a consequence.
Insomnia — promising, but thin on evidence
The sleep data is suggestive but not yet robust enough to make strong claims. The best numbers come from the 2023 anxiety meta-analysis, which found large improvements in comorbid insomnia in anxious patients (ES = −1.02 across 3 trials) — though this is an indirect finding embedded in an anxiety meta-analysis, not a primary insomnia study.[3] A 2025 real-world observational study of 60 participants reported 48% achieved insomnia remission after 21 days of home Alpha-Stim use, with improvements corroborated by actigraphy data.[7] However, a 2024 RCT in subclinical insomnia found no significant improvement in sleep outcomes over sham — only improvements in depression and physical well-being.[8]
The emerging picture: CES may meaningfully help with sleep when insomnia is anxiety-driven, but it is not yet established as a standalone insomnia treatment.
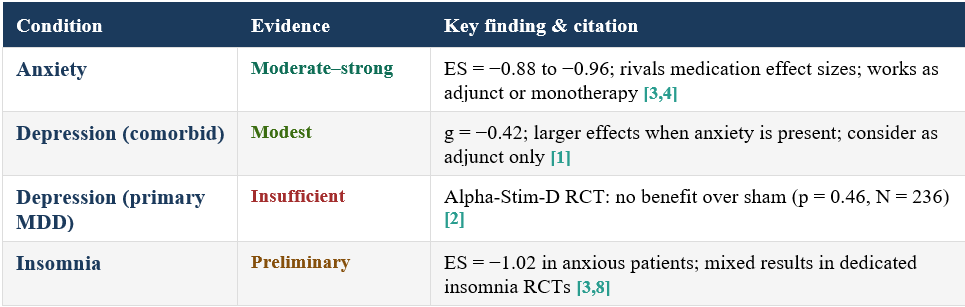
Condition-by-condition summary
What is the mechanism of action?
Mechanism research in CES is honest about its limits — and that honesty is actually reassuring compared to fields that overclaim. Three plausible frameworks exist, none definitively proven in humans:
1. Neurotransmitter modulation
Animal studies and some human trial data suggest CES increases serotonin, norepinephrine, dopamine, and GABA — the same neurotransmitter systems targeted by antidepressants and anxiolytics, via a completely different route. CES may also increase endorphin release, potentially explaining a portion of the anxiolytic effect.[10]
2. Autonomic nervous system effects
One influential theory proposes that earlobe electrodes stimulate afferent vagus nerve branches, shifting the nervous system toward parasympathetic dominance. A 2023 randomized controlled study found CES flattened the cortisol awakening response and altered bedtime cortisol levels — consistent with modulation of HPA axis reactivity, though direct vagal stimulation evidence remains indirect.[11]
3. Brain network and EEG modulation
EEG studies show CES reduces high-frequency alpha and beta power associated with arousal and anxiety, producing patterns that resemble meditation states. fMRI data demonstrates modulation of the default mode network — the circuit most associated with rumination and self-referential thinking. Computational modeling suggests current from earlobe electrodes reaches cortical and subcortical structures at subthreshold neuromodulatory intensities.[10,11]
The honest answer
No one can tell you with certainty why CES works when it works. The three frameworks above are plausible, overlapping, and not mutually exclusive. This is not unusual in psychiatry — despite decades of use, the precise mechanisms of SSRIs remain incompletely understood as well.
The real methodological problems: why hold your enthusiasm in check
A 2021 critical review identified severe methodological problems across the CES literature that any reader should understand.[12] These are not minor quibbles:
• Blinding is very hard with CES. Sham devices feel different from active ones. When participants detect whether they received real stimulation, their expectations shape their outcomes — inflating effect sizes in the active group. Very few CES trials have verified that blinding actually held.
• Much of the positive literature is manufacturer-funded. A disproportionate share of Alpha-Stim research has been funded by or conducted in collaboration with Electromedical Products International. Independent trials — including the Alpha-Stim-D study — have produced less favorable results.[2,12]
• Parameters vary wildly across studies. Frequency, current intensity, session duration, and number of sessions differ enormously across trials and are often incompletely reported.[12] This makes it nearly impossible to know what protocol actually drives benefit — or to replicate it.
• Publication bias may be present. Positive small trials get published; negative small trials often do not. When the largest, most rigorous, independently funded trial produces a flat result,[2] this is the corrective signal that meta-analyses of smaller studies missed.
The safety picture: one genuine advantage
Where CES has a clear edge
Across the published literature, CES has produced no serious adverse events. The most common side effect is mild ear discomfort or skin irritation at the electrode sites. Dropout rates in active groups are no higher than in sham groups across meta-analyses.[1,3,4]
Compare this to antidepressants: nausea affects roughly 1 in 6 people on duloxetine, sexual dysfunction is common with SSRIs and SNRIs, and discontinuation syndromes are well-documented.[13] For medication-averse individuals, the safety and tolerability advantage of CES is clinically meaningful — even if its efficacy remains uncertain.
Standard cautions: CES should not be used with cardiac pacemakers or other implantable electrical devices. Data in pregnancy is absent. Metal implants near the head or neck warrant discussion with a physician. These are not absolute prohibitions, but they are conversations worth having before purchase.
So — is it worth it?
That depends entirely on what you are hoping it will do.
The bottom line
For anxiety: The evidence is genuinely reasonable. Effect sizes compare favorably with first-line medications.[3,4,6] A structured 3–5 week trial is worth considering, especially for medication-averse individuals or as an adjunct to therapy.
For depression (primary MDD): Not a standalone treatment. The Alpha-Stim-D Lancet Psychiatry trial was well-powered and negative.[2] Do not use CES as a substitute for antidepressants or evidence-based psychotherapy for primary major depression.
For depression (comorbid): A limited adjunct role is plausible when depression is comorbid with anxiety.[1] Do not position CES as a substitute for evidence-based care.
For insomnia: Worth considering when insomnia is anxiety-driven.[3,7] Insufficient dedicated RCT evidence to recommend as a standalone sleep intervention.[8]
For everyone: If you try it, use it for a defined period (3–5 weeks), with a specific outcome in mind, and track it with a validated scale (GAD-7, PHQ-9, ISI). This converts an open-ended supplement purchase into a trackable intervention with a clear decision point.
If you are a clinician: Being familiar with the evidence and being able to say “here is where I think it may help, here is where I think the data is weak” is far more useful than dismissal or uncritical enthusiasm.
If you are a patient or consumer: The anxiety data is real enough to take seriously. The depression data is not.
References
[1] Liu, S. Y., Chen, R., & Wang, C. H. (2025). Efficacy of cranial electrotherapy stimulation for treating primary and secondary depression in adults: A meta-analysis of randomized controlled trials. Journal of Affective Disorders, 382, 488–497. https://doi.org/10.1016/j.jad.2025.04.074
[2] Morriss, R., Patel, S., Boutry, C., et al. (2023). Clinical effectiveness of active Alpha-Stim AID versus sham Alpha-Stim AID in major depression in primary care in England (Alpha-Stim-D): A multicentre, parallel group, double-blind, randomised controlled trial. The Lancet Psychiatry, 10(3), 172–183. https://doi.org/10.1016/S2215-0366(23)00007-X
[3] Chung, F. C., Sun, C. K., Chen, Y., et al. (2023). Efficacy of electrical cranial stimulation for treatment of psychiatric symptoms in patients with anxiety: A systematic review and meta-analysis. Frontiers in Psychiatry, 14, 1157473. https://doi.org/10.3389/fpsyt.2023.1157473
[4] Ching, P. Y., Hsu, T. W., Chen, G. W., et al. (2022). Efficacy and tolerability of cranial electrotherapy stimulation in the treatment of anxiety: A systematic review and meta-analysis. Frontiers in Psychiatry, 13, 899040. https://doi.org/10.3389/fpsyt.2022.899040
[5] Cipriani, A., Furukawa, T. A., Salanti, G., et al. (2018). Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: A systematic review and network meta-analysis. The Lancet, 391(10128), 1357–1366. https://doi.org/10.1016/S0140-6736(17)32802-7
[6] Gosmann, N. P., Costa, M. A., Jaeger, M. B., et al. (2021). Selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors for anxiety, obsessive-compulsive, and stress disorders: A 3-level network meta-analysis. PLOS Medicine, 18(6), e1003664. https://doi.org/10.1371/journal.pmed.1003664
[7] da Silva, K. M., Broom, C., Daly, H., et al. (2025). Real-world evaluation of at-home cranial electrotherapy stimulation (CES) for the management of sleep, anxiety, depression, stress, quality of life, and self-efficacy. Journal of Affective Disorders. https://doi.org/10.1016/j.jad.2025.120859
[8] Hong, J. K., & Yoon, I. Y. (2024). Efficacy of cranial electrotherapy stimulation on mood and sense of well-being in people with subclinical insomnia. Journal of Sleep Research, 33(1), e13978. https://doi.org/10.1111/jsr.13978
[9] Cheng, Y. C., Kuo, P. H., Su, M. I., & Huang, W. L. (2022). The efficacy of non-invasive, non-convulsive electrical neuromodulation on depression, anxiety and sleep disturbance: A systematic review and meta-analysis. Psychological Medicine, 52(5), 801–812. https://doi.org/10.1017/S0033291721005560
[10] Kavirajan, H. C., Lueck, K., & Chuang, K. (2014). Alternating current cranial electrotherapy stimulation (CES) for depression. Cochrane Database of Systematic Reviews, 7, CD010521. https://doi.org/10.1002/14651858.CD010521.pub2
[11] Lee, M., Kim, Y., Yoon, I. Y., & Hong, J. K. (2023). Effects of cranial electrotherapy stimulation on improving depressive symptoms in people with stress: A randomized, double-blind controlled study. Journal of Affective Disorders, 340, 835–842. https://doi.org/10.1016/j.jad.2023.08.062
[12] Brynyé, T. T., Patterson, J. E., Wooten, T., & Hussey, E. K. (2021). A critical review of cranial electrotherapy stimulation for neuromodulation in clinical and non-clinical samples. Frontiers in Human Neuroscience, 15, 625321. https://doi.org/10.3389/fnhum.2021.625321
[13] Simon, G. E., Moise, N., & Mohr, D. C. (2024). Management of depression in adults: A review. JAMA, 332(2), 141–152. https://doi.org/10.1001/jama.2024.5756
Disclaimer: This article is intended for educational purposes and does not constitute medical advice. It does not replace individualized clinical judgment or a relationship with a licensed healthcare provider. Clinicians should apply findings within the context of each client’s overall treatment plan.
RxPsychology: Mind and Medicine © 2026